HRT Made My Breasts Dense — Do I Need to Stop Taking It?
I want to tell you about a patient I saw a couple of weeks ago.
She came in holding a letter from the radiology service — her mammogram result. She'd been on HRT for two years. Hot flushes gone. Sleep restored. She felt like herself again for the first time since her early fifties.
Then she got her radiology report.
It said her breast density was Category C — heterogeneously dense. And somewhere between reading that letter and sitting in my consulting room, she had already decided she needed to stop her HRT.
She hadn't spoken to her GP. She hadn't contacted me. She had just decided.
Because the letter said dense breasts. She knew — the way we all kind of know, from something we read once, or a friend who said something — that dense breasts mean higher cancer risk. It must be that HRT caused the density. Therefore HRT was causing cancer risk. So she needed to stop.
That reasoning is not crazy. It is completely understandable. But it is also not the full picture.
What breast density actually is
A mammogram does not just look for lumps. It also reports on the composition of your breast tissue — specifically, the ratio of glandular and fibrous tissue to fatty tissue. We call this breast density.
There are four categories. Category A is almost entirely fatty — the mammogram looks dark, and reading it is relatively straightforward. Category D is extremely dense — the mammogram looks very white, and it can be technically harder to detect abnormalities within all that white tissue. Most women fall somewhere in the middle, in Category B or C.
KEY POINT
Breast density is not a pathology. It is not a disease. It is not a tumour. It is a description of the composition of your tissue — the same way someone might describe you as having thick hair or fine hair. It is a characteristic.
Dense breast tissue does do two things that are clinically relevant. First, it can make mammograms harder to read — dense tissue and early cancers can both appear white on a mammogram, which is why women with dense breasts may be offered additional imaging in some screening programmes. Second, independently of HRT, higher breast density is associated with a modestly increased lifetime risk of breast cancer.
That word — modestly — matters enormously. Because by the time it reaches a patient letter, "modestly increased risk associated with dense breasts" has often become "dense breasts cause cancer." And those are very different statements.
What the research actually shows about density and cancer risk
To put numbers to this: women with extremely dense breasts (Category D) have roughly twice the breast cancer risk of women with average density. Women with Category C density have approximately one and a half times the average risk.
For context, the average lifetime breast cancer risk for a woman in the general population is around 12.5% — the one-in-eight figure you may have heard. Here is what that looks like across the four categories:
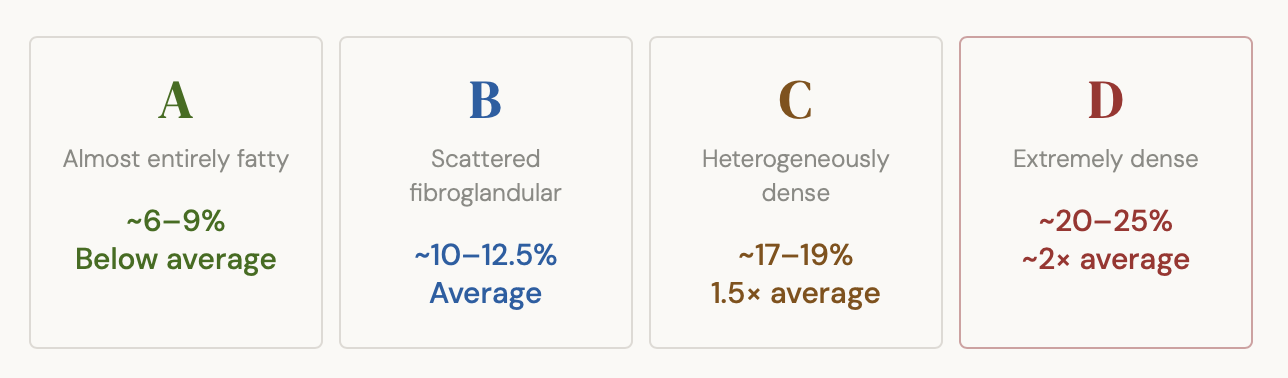
That is a real difference. It is worth knowing. But it is not a one-in-three or one-in-two risk. It is a nudge upward, not a cliff edge. And density doesn't exist in isolation — it sits alongside your age, family history, previous breast biopsies, weight, alcohol use, and yes, your HRT.
Does HRT cause breast density — and does that matter?
Yes, in some women, HRT — particularly combined oestrogen and progestogen — can increase breast density. This is well established in the literature. But here is what the mammogram letter does not tell you: not all HRT is the same.
The type of progestogen matters enormously. Synthetic progestogens — called progestins — which are used in some combined oral HRT preparations, have a greater tendency to increase breast density than body-identical progesterone, also called micronised progesterone. Body-identical progesterone, when taken orally or vaginally, has a much lower association with breast density change and a better safety profile when it comes to breast cancer risk overall.
Your mammogram letter does not know which type of HRT you are on. It cannot tell. It just sees density. And that is why reading a mammogram report without clinical context can be genuinely misleading.
HRT-INDUCED DENSITY IS NOT THE SAME AS NATURALLY OCCURRING DENSITY
This is the nuance that most patients — and, frankly, some letters — miss entirely.
Research has shown that HRT-induced density changes often involve fluid shifts and stromal oedema rather than a true increase in glandular cell mass. That distinction matters, because naturally occurring dense breast tissue carries its risk partly through having more epithelial cells — the actual substrate for malignant transformation.
HRT-induced density is also largely reversible when HRT is stopped, typically within three to six months. Naturally occurring density does not reverse in the same way. Studies suggest that density-related changes account for only around 10% of HRT's excess breast cancer risk — the majority of that risk operates through direct hormonal effects on breast tissue, not through the density itself.
BOTTOM LINE
For most women using HRT for a defined period, the absolute risk increase remains small — and stopping HRT has its own real costs: return of hot flushes, sleep disruption, joint pain, mood changes, and accelerated bone density loss. That trade-off deserves a proper conversation.
The screening question
In New Zealand, the BreastScreen Aotearoa programme invites women aged 45 to 69 for two-yearly mammograms. Dense breast tissue is common in this age group and is routinely detected.
For women with very high density (Category D), or those with additional risk factors such as a strong family history, a personal history of breast cancer, or a known genetic mutation, additional imaging such as ultrasound or MRI may be appropriate. This is a conversation to have with your GP or specialist — not a conclusion to draw from the letter alone.
One imaging advancement worth knowing about is tomosynthesis — sometimes called 3D mammography. Because it takes layered images rather than a flat image, it reduces the white-on-white masking problem that makes dense breasts harder to read. In Category C and D breasts, tomosynthesis can add meaningfully to sensitivity. It is not universally available in New Zealand at present, but it is increasingly used in private radiology and worth asking about.
For most women on HRT with Category C density — the most common finding — the standard recommendation is not to stop HRT and not to assume that additional screening is automatically required. It is to continue with regular mammography and to have a clinical conversation about your individual risk profile.
Five questions to ask your doctor
Clinical appointments are short. If you are on HRT and you receive a mammogram report commenting on breast density, take these questions with you.
What type of HRT am I on, and does it affect breast density?
If you are on a combined preparation with a synthetic progestogen and density is a concern, it may be worth discussing whether switching to body-identical progesterone is appropriate for you. This is not always possible — but it is a legitimate conversation to have.
What category is my density, and what does it mean for my screening?
Category B is common and generally requires no change. Category C warrants conversation. Category D may warrant additional imaging depending on your overall risk profile.
What is my overall breast cancer risk?
Density is one factor. Age, family history, personal history, weight, alcohol use, and duration of HRT use all contribute. No single factor tells the full story. Ask for your risk to be considered in context.
What would stopping HRT cost me?
This is the question women often do not think to ask, because they are focused on the density finding. But it is the other side of the equation. That cost needs to sit alongside the risk when you make a decision.
What is the plan going forward?
What is the monitoring interval? When is the next mammogram? Under what circumstances should you come back sooner? Leave with a clear plan, not just a conversation.
You are allowed to ask all of these questions. You are allowed to take notes. You are allowed to bring someone with you. You are allowed to say: I need a moment before I decide anything.
What I want you to take away from this
The patient I told you about at the start — we sat together for about 25 minutes. I explained what Category C density means. I looked at her specific HRT formulation. I went through her family history, her personal history, her overall risk profile.
At the end of that conversation, she decided to stay on her HRT — with a plan to switch to body-identical progesterone at her next prescription review, and to continue with annual mammography rather than two-yearly.
It was a different decision to the one she had almost made alone in her kitchen. Not because I talked her out of anything. But because she now had the full picture.
The evidence on HRT and breast density is more nuanced than a mammogram letter can convey. Your decision — whatever it is — should be made with the full picture. You deserve that conversation. Make sure you get it.