Why Two Women Can Have the Same Breast Cancer Diagnosis — and Completely Different Treatment Plans
Two women walk out of the same hospital with the same three words on their pathology report. One is told she needs chemotherapy before surgery. The other is booked straight in for an operation. Their treatment plans look nothing alike — and nobody has explained why.
If you've been in that position, or you're supporting someone who has, that gap between what you're told and what you actually need to understand can feel deeply unsettling. You start to wonder whether someone has made a mistake. Whether you're getting the right plan. Whether the system is failing you.
It isn't. And once you understand what's actually driving these decisions, the confusion tends to lift — and something more useful takes its place.
Breast cancer is not one disease

This is the single most important thing I want you to take away from this post, and it's something I wish every woman heard on the day of her diagnosis.
Breast cancer is not one disease. It's a family of diseases that all happen to start in the breast tissue — but underneath, they behave very differently. And the single biggest thing that separates them is something called receptor status.
Think of receptors like locks on the outside of a cancer cell. We test for three of them: oestrogen receptors (ER), progesterone receptors (PR), and HER2, which is a growth protein receptor. These locks tell us what the cancer is feeding on — and that tells us which treatments will actually work, because the treatment has to match the lock.
A cancer fuelled by oestrogen responds to hormone-blocking therapy. A HER2-driven cancer can be targeted with very specific drugs that go directly after that receptor. A cancer with none of these receptors — what we call triple negative — needs a completely different approach again.
If you know your receptor status, you already understand more about your cancer than most women do on the day they're diagnosed. That's not a small thing. It's the foundation of your entire treatment plan.
The second layer: how fast is it moving?
Receptor status tells us what kind of cancer it is. Tumour grade tells us how urgently your team needs to act.
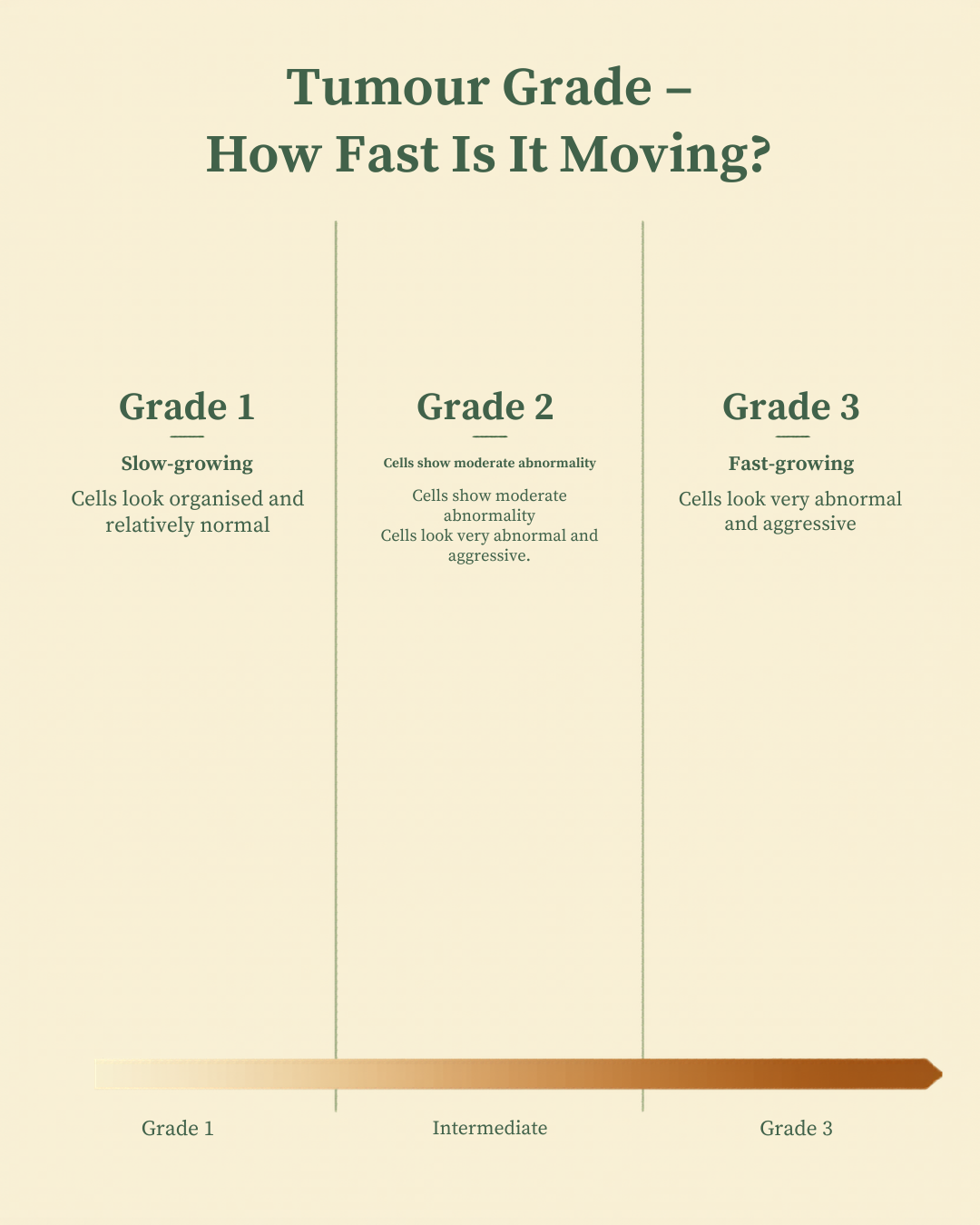
Grade describes how abnormal the cancer cells look under a microscope compared to normal breast tissue. Grade 1 cells look relatively organised — slow-growing, less aggressive. Grade 3 cells look very abnormal and are fast-moving. Grade 2 sits somewhere in between.
Grade doesn't change your receptor status, but it absolutely influences the urgency of treatment and sometimes the type of chemotherapy that's recommended. A grade 3 triple negative cancer behaves very differently to a grade 1 hormone receptor positive cancer — even when both are caught at the same stage.
Your oncologist isn't looking at one number in isolation. They're building a picture from several pieces of information together. When you understand that, the treatment plan stops feeling random and starts making sense.
Genomic testing: your tumour's own roadmap
There's a third piece of this puzzle that not everyone will need — but for the right patient, it can be one of the most clarifying pieces of information in the entire treatment journey.
It's called genomic testing, and the most commonly used version in breast cancer is the Oncotype DX score. This test is done after surgery, on the tumour tissue that's been removed. It's not a blood test. It analyses the activity of specific genes within your actual tumour and answers two questions: how likely is recurrence, and will chemotherapy actually reduce that risk?
Not everyone is a candidate. The test is most useful for women with hormone receptor positive cancer — ER positive, PR positive, HER2 negative — with lower grade tumours, at stage 1 or 2, and either no lymph node involvement or up to three nodes affected.
If you fit that profile, this score can genuinely change the conversation. A low score tells your oncologist that chemotherapy is unlikely to add meaningful benefit — and you can be spared treatment you didn't need. A high score tells them the tumour biology is active enough that adding chemotherapy is likely worth it.
This is not guesswork. It's your tumour's own genetic activity helping to guide the decision — and it's one of the most powerful examples of personalised medicine we have in breast cancer right now.
One important note for New Zealand readers: the Oncotype DX test is currently self-funded here, unlike in the UK where it's publicly funded. That's a conversation worth having with your oncologist before you assume it's not available to you.
Why some women have chemotherapy before surgery
Once you understand receptor status and grade, the treatment sequence starts to make a lot more sense — including the question that comes up constantly: why do some women have chemotherapy first?
This is called neoadjuvant chemotherapy, and it's not a sign that things are more serious. It's a deliberate, strategic choice.
For HER2 positive and triple negative breast cancers in particular, giving chemotherapy before surgery can shrink the tumour — sometimes significantly. That can mean a smaller operation. It can mean the difference between a mastectomy and a lumpectomy. And in some cases, when we get to surgery and look at the tissue, the cancer has responded so well that there's very little — or even no — remaining disease left. We call that a pathological complete response, and it's a genuinely meaningful result.
There's another advantage to treating first. It lets us see, in real time, how your specific cancer responds. If it responds well, that's valuable information. If it doesn't respond as expected, we can adjust. That's something we can't do if we go straight to surgery.
So if you've been told you're having chemotherapy before your operation — that is not a worse path. In many cases, it's the smarter one.
Hormone receptor positive cancer: surgery first, then what?
For women with hormone receptor positive, HER2 negative cancer — the most common subtype — the sequence tends to look different. Surgery usually comes first, and the cornerstone of treatment is hormone therapy: drugs like tamoxifen or aromatase inhibitors that reduce the oestrogen available to fuel the cancer cells. These are taken for years — typically five to ten — and for many women, hormone therapy alone is highly effective.
The question that has to be answered after surgery is whether this particular patient also needs chemotherapy on top of hormone therapy. That's where the Oncotype DX score, for eligible patients, becomes so valuable. It takes a genuinely difficult clinical question and grounds it in the biology of your specific tumour.
Why two women with identical biology can still get different recommendations
Sometimes women go through all of this — they understand their receptor status, their grade, they've had the genomic testing conversation — and they still end up with a different recommendation to someone with a very similar diagnosis. This is where it's worth being clear: treatment isn't just about the cancer. It's about the person who has it.
Age matters. Fertility wishes matter. Pre-existing health conditions matter. A woman in her mid-thirties who wants to preserve fertility has considerations that are genuinely different from a woman in her sixties who doesn't. A patient with pre-existing heart disease needs a different chemotherapy protocol to a patient with a healthy cardiovascular system, because some drugs carry cardiac risks that have to be weighed carefully.
And your values matter too. Some women want the most aggressive option available. Others want to balance effectiveness with quality of life through treatment. Neither of those is wrong. A good oncology team will ask about both — because good oncology is not just about treating a tumour. It's about treating a person who happens to have one.
How your treatment plan is actually made
Most women assume their oncologist sits alone in an office, reviews the scan, and decides. That's not what happens.
Every breast cancer patient's case is reviewed by a multidisciplinary team — an MDT. This is a group of specialists who come together to review your case: your breast surgeon, your medical oncologist, your radiation oncologist, the pathologist who read your biopsy, a radiologist, and sometimes a geneticist. They look at the images, the pathology, the receptor status, the grade, and where relevant the genomic score — and they arrive at a recommendation together.

This is why it can feel like it takes time to get your treatment plan. It's not the system being slow. It's the system being thorough — on your behalf. And if you're ever unsure whether your case went to an MDT, that is absolutely a question you are entitled to ask.
Three questions to take to your next appointment
Understanding all of this is only useful if you can walk into your next appointment and use it. These are the three questions I'd want you to have ready.
"What is my full receptor status — ER, PR, and HER2 — and what does that mean for the treatments most relevant to me?" This anchors the conversation in your specific biology, not a general discussion about breast cancer.
"Am I a candidate for genomic testing, and how would the result change my treatment recommendation?" If you're hormone receptor positive and HER2 negative, this is especially important to ask. Not every patient needs this test — but you deserve to know whether you're one who does.
"Has my case been reviewed by the full multidisciplinary team?" Not because you doubt your doctor. But because you understand that the best decisions are collaborative ones — and you want to know that process has happened for you.
Write those down. Take them in. You are not being difficult. You are being informed.
The bottom line
Go back to those two women walking out of the same hospital with the same three words on their pathology report.
Same diagnosis. Different receptor status. Different grade. Different genomic scores. Different ages, different health histories, different values about their own care.
Of course their treatment plans looked different. They should look different. Because they are different women, with different cancers, who deserve a plan built around them — not a one-size-fits-all approach.
That's not the system failing. That's the system working exactly as it should.
If you'd like to go deeper, I've made a companion video walking through exactly what your biopsy report is telling you — term by term, in plain language. Words like "moderately differentiated," "Ki67," and "lymphovascular invasion" mean something specific, and understanding them will help you have a much better conversation at your next appointment. You'll find it on my YouTube channel.